

Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma (NHL), constituting 25% of NHL cases (Teras, 2016). Although survival rates have improved, with a 5-year relative survival of 63.8% in the United States (SEER Cancer Statistics, 2018), outcomes in DLBCL remain heterogeneous with inferior survival amongst some patient subgroups. Racial and ethnic disparities in access to care and outcomes are well-established and are critical issues across a number of malignancies, including NHL (Shenoy, 2011; Griffiths, 2010). The purpose of this study was to assess for racial and ethnic differences in patient and disease characteristics at diagnosis, and in outcomes for patients diagnosed with DLBCL within the Veterans Health Administration (VHA), where access to care may be less susceptible to other socioeconomic factors.
Methods
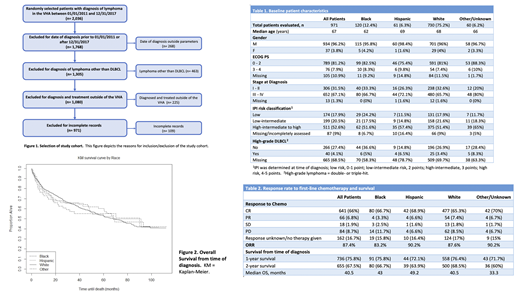
Trained abstractors performed a retrospective chart review of 2036 randomly selected patients seen in the VHA nationwide who were diagnosed with lymphoma between 01/01/2011 and 12/31/2017. We included patients diagnosed with DLBCL and excluded patients based on the criteria in Figure 1. We evaluated baseline patient and disease characteristics, including Eastern Cooperative Oncology Group (ECOG) performance status, stage at diagnosis, International Prognostic Index (IPI) score, pathology reports to identify high-grade lymphomas, and response to first-line treatment.
Results
A total of 971 patients met inclusion criteria for analysis. Patients were predominantly male, white, had a median age of 67, and presented primarily with advanced disease (Table 1). Patients in each subgroup presented with similar rates of stage III and IV disease, with no statistically significant difference in stage at presentation amongst each racial subgroup (white vs black, P=0.85; white vs Hispanic, P=0.30; white vs other, P=0.11). Most patients in each racial/ethnic group had a good performance status at diagnosis, with ECOG 0-2 in 75.4 - 82.5% of patients in each subgroup.
The entire study population had an objective response rate (ORR) of 87.4% (complete response (CR) rate 66%) (Table 2). Response rates were similar across the 4 subgroups, with the majority of patients achieving a complete response (CR) after first-line therapy (66.7%, 68.9%, 65.3%, and 70% for black, Hispanic, white, and other/unknown patients, respectively). There were no statistically significant differences in ORR amongst subgroups (white vs black, P=0.28; white vs Hispanic, P=0.75; white vs other, P=0.75).
Median overall survival (OS) from the time of diagnosis was 40.5 months for the entire study population (Table 2). OS rates were similar regardless of race with a median OS of 43 months for black patients, 49.2 months for Hispanic patients, 40.5 months for white patients, and 33.3 months for other/unknown patients (Figure 2). There was no statistically significant difference in median OS between subgroups (white vs black, P= 0.84; white vs Hispanic, P=0.39; white vs other, P=0.18). The 1-year survival rates were similar at 75.8%, 72.1%, 76.4%, and 71.7% for black, Hispanic, white, and other/unknown patient subgroups, respectively. Between 60 - 68.5% of patients in each subgroup remained alive at 2 years, with no significant differences in survival rates at 1 or 2 years.
Conclusions
In this retrospective study of patients diagnosed with DLBCL in the VHA nationwide, we found that there were no statistically significant differences in baseline patient characteristics at diagnosis or in response rates to first-line chemotherapy, 1- and 2-year OS rates, or median OS amongst each racial subgroup. Potential limitations of this study include that the population is predominantly male and therefore, may not be applicable to the female population, and that there was missing/incomplete data for pathologic assessment of high grade lymphoma in 68.5% of our population, which could provide important data about expected outcomes. Further studies with a longer follow-up period are needed to help characterize potential differences in outcomes and relapse rates. Our data suggest that when standard of care therapy is given equally to patients with DLBCL, similar outcomes occur for black, Hispanic, and white patients. The development of interventions to address healthcare disparities and to ensure access to appropriate and timely care for all patient populations is of paramount importance.
No relevant conflicts of interest to declare.

